If you’ve spent any time researching light therapy, you’ve almost certainly run into a wall of terminology. Cold laser. LLLT. Photobiomodulation. Low-level laser therapy devices. They sound different, they’re marketed differently, and yet they’re all describing variations of the same underlying science. Then you start looking at actual products – handheld devices, panels, wearable wraps, transcranial headsets – and the confusion compounds quickly.
By the end, you’ll know exactly what these devices are, how laser-based models differ from LED devices (a distinction that matters more than most people realize), which formats are best suited for different needs, and the key features that separate a worthwhile investment from one that’s likely to disappoint.
What “Cold Laser,” “LLLT,” and “Photobiomodulation” Actually Mean
Let’s settle the terminology first, because this trips up almost everyone.
Low-level laser therapy (LLLT), cold laser therapy, and photobiomodulation (PBM) are three names for the same category of treatment. They all refer to the application of low-power red or near-infrared light to tissue to stimulate biological processes – without generating heat, cutting tissue, or causing damage.
The word “cold” in cold laser therapy doesn’t mean the device is cold to the touch. It means the laser operates at a power level low enough that it doesn’t heat tissue. This distinguishes it from surgical or ablative lasers – CO₂ lasers, for example – which deliberately destroy or reshape tissue and require significant downtime. Cold laser devices stimulate without damaging. That’s the entire point.
The term “photobiomodulation” is now preferred in the scientific literature because it’s more accurate – it describes what’s actually happening (light modulating biological activity) rather than just the device type. You’ll see LLLT used more in older research and in clinical settings; PBM is the more modern standard.
All three terms are legitimately interchangeable as a category. The confusion comes when people use them to mean specific things – which brings us to the device question.
Laser vs. LED: The Distinction That Actually Matters
Here’s where things get genuinely important, because the market mixes these up constantly.
Not all “LLLT devices” or “cold laser devices” are the same. Some use actual laser diodes. Others use LEDs. The biological goal is identical – photobiomodulation – but the physical properties of the light are meaningfully different.
True laser light is:
- Coherent – the light waves travel in phase with each other
- Collimated – it travels in a tight, non-diverging beam
- Monochromatic – it emits a very precise, narrow wavelength (often 1–2 nm bandwidth in diode lasers)
LED light is:
- Non-coherent – waves travel out of phase
- Divergent – spreads out as it travels
- Broader bandwidth – typically 20–30 nm spread around the target wavelength
The practical consequence is penetration depth. Laser light, because it’s coherent and collimated, penetrates deeper into tissue before scattering – up to 2–5 cm in clinical devices. LED light, because it diverges and scatters more quickly, primarily affects superficial tissue.
That said, the distinction is more nuanced than a simple “lasers are better” conclusion. A 2018 review in Photochemical & Photobiological Sciences by Heiskanen and Hamblin noted that coherence is largely lost as light scatters through biological tissue anyway – which suggests that for many applications, the wavelength and delivered dose matter more than whether the source is a laser or an LED. What this means practically: for surface-level treatments like skin rejuvenation, acne, and wound healing, quality LED devices can match laser outcomes. For deep tissue targets – joints, tendons, muscle bellies, and certainly the brain – true laser devices have a meaningful penetration advantage.
“LLLT and red light therapy operate on similar photobiomodulation principles,” explains Dr. Ellie Rashid, consultant dermatologist at London’s OneWelbeck. “However, LLLT typically refers to the use of focused laser light at specific wavelengths, whereas red light therapy often includes broader-spectrum LED devices.”
The takeaway: when you see a product marketed as a “cold laser therapy device,” check whether it actually uses laser diodes or LEDs. Both can work well – but for different targets, and at different price points.
How Do These Devices Work?
Whether the source is a laser or an LED, the biological mechanism is the same. Photons at specific wavelengths in the red (620–700 nm) and near-infrared (700–1100 nm) range penetrate tissue and are absorbed by chromophores inside cells – primarily cytochrome c oxidase, an enzyme in the mitochondrial electron transport chain.
This absorption triggers a cascade of effects:
- Increased ATP production – cells have more energy to repair, regenerate, and function optimally
- Reduced oxidative stress – PBM modulates reactive oxygen species (ROS), reducing cellular damage
- Cytokine modulation – pro-inflammatory signaling molecules (TNF-α, IL-1β, IL-6) are downregulated; anti-inflammatory factors are upregulated
- Nitric oxide release – improves local circulation by dilating blood vessels
- Nerve modulation – reduces pain signal transmission at the nerve level
The research backing these mechanisms is substantial.The key variables that determine outcome are wavelength, power density (irradiance), total energy delivered per session (dose in J/cm²), and treatment frequency. Get these right and the therapy works. Get them wrong – too little, too much, or wrong wavelength for the target tissue – and it doesn’t.
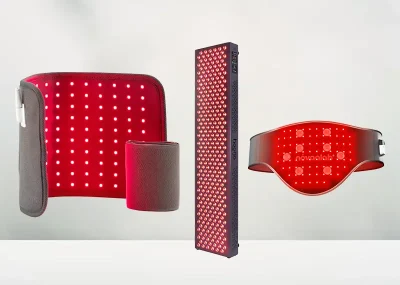
The Main Device Formats: What Each One Is For
The photobiomodulation device market has expanded significantly beyond simple handheld probes. Here’s a breakdown of every major format, what it’s best suited for, and where its limitations lie.
Handheld Cold Laser Devices
The original clinical format. A pen- or gun-shaped device with one or a small cluster of laser diodes, used to treat a specific point or small area with high precision.
These are the devices most likely to use true laser diodes rather than LEDs – making them the best choice for deep tissue targets. Most operate at 650 nm (red) and 808 nm (near-infrared), often delivering both simultaneously. Output power typically ranges from 100 mW to 500 mW for consumer devices; professional clinical units can exceed 1,000 mW.
A good example is the handheld NOVAA Light Switch, which combines both LED and laser diodes to provide broad surface coverage while delivering more targeted light to deeper tissues.
- Best for: Targeted joint pain, tendon injuries, nerve pain, trigger points, small surface area treatments, sports injury recovery, and applications where red light therapy for tendonitis and wound healing may help support tissue repair and recovery Also the format most used in veterinary cold laser therapy.
- Limitations: Small treatment area means longer sessions when multiple areas need treating. Requires precise positioning to be effective. Higher-powered clinical units may require professional supervision.
- Who uses them: Physical therapists, chiropractors, sports medicine professionals, and increasingly, home users managing chronic joint or nerve conditions.
LED Panels and Pads
Large arrays of LEDs arranged in flat panels or flexible pads. These are what most people mean when they say “red light therapy device.” They cover large surface areas efficiently and are the most accessible format for home use.
Modern professional-grade LED panels can achieve irradiance levels (50–100 mW/cm²) comparable to LLLT devices at a given distance – the difference is they deliver that energy over a much larger area rather than a focused point. This makes them ideal for broad-coverage applications but less suited to deep, targeted treatment.
Best for: Skin rejuvenation, wound healing, hair growth, muscle recovery, full-body anti-inflammatory protocols, broad-area pain management. The format most studied for skin-related applications.
Limitations: Limited penetration depth compared to laser devices. Less effective for deep joint structures unless near-infrared wavelengths are included. Device quality varies enormously – irradiance claims are frequently overstated by manufacturers.
Who uses them: Broad consumer market – skin health, anti-aging, general wellness, and recovery-focused users.
Transcranial Photobiomodulation devices
The most specialized – and arguably most interesting – category. Transcranial PBM (tPBM) devices deliver near-infrared light through the skull to directly stimulate brain tissue. The target is the same mitochondrial cytochrome c oxidase pathway, but in neurons rather than musculoskeletal tissue.
The science here is still developing but moving quickly. A 2023 systematic review in Ageing Research Reviews analyzed 35 human studies and found 82.9% reported positive cognitive outcomes from tPBM. A 2025 randomized controlled trial published in the Journal of Affective Disorders found significant hypnotic (sleep-improving) effects in a wearable tPBM device, though antidepressant effects were not confirmed.
The preferred wavelengths for transcranial applications are 810 nm and 1064 nm – the latter offering superior skull penetration due to lower scattering and absorption by hemoglobin and water.
Best for: Cognitive enhancement, traumatic brain injury recovery support, sleep improvement, mood support, and emerging research into neurodegenerative conditions including Alzheimer’s and Parkinson’s.
Limitations: Consumer devices are limited in power compared to clinical laser systems. The field is still establishing standardized protocols. Devices are expensive relative to other PBM formats. Not a replacement for medical treatment of serious neurological conditions.
Who uses them: Biohackers, TBI recovery patients, people exploring non-pharmacological cognitive support, and clinical researchers.
MOST POPULAR IN HEALTH




What These Devices Are Clinically Used For
The evidence base for photobiomodulation spans a surprisingly wide range of conditions. Here’s where the research is strongest:
Musculoskeletal pain and injury – The most studied application. Clinical trials consistently show 30–50% reductions in pain scores for osteoarthritis, tendinopathy, neck pain, and lower back pain after 4–6 weeks of treatment. A 2024 MDPI review of LLLT confirmed meaningful benefit for muscle recovery and rehabilitation, with particular strength for subacute soft tissue injuries.
Wound healing – PBM accelerates healing of diabetic foot ulcers, surgical wounds, and oral mucositis (a common and painful side effect of cancer chemotherapy).
Hair loss – Well-supported by clinical evidence for androgenetic alopecia (pattern baldness). Multiple systematic reviews confirm increased hair density and thickness with consistent use of both laser and LED devices in the therapeutic window. Devices like the Hooga Red Light Therapy Laser Helmet are designed to deliver targeted scalp coverage for at-home use.
Skin rejuvenation and acne – Red light (630–660 nm) stimulates collagen production and reduces acne-causing bacteria via blue light (when included). These are among the most commercially accessible applications.
Dental and oral health – A 2025 evidence-based guidelines paper in Bioinformation Journal confirmed PBM’s role in managing oral mucositis, temporomandibular disorder pain, orthodontic discomfort, and implant healing.
Cognitive and neurological support – Still emerging but showing genuine promise. The tPBM research pipeline includes studies on TBI recovery, Alzheimer’s, Parkinson’s, depression, and cognitive enhancement in healthy adults.
How to Choose the Right Device
The right device depends almost entirely on what you’re trying to treat. Here’s a practical framework:
For deep joint or tendon pain – prioritize a true laser device (not just LEDs) with near-infrared wavelengths at 808–850 nm. Handheld cold laser devices or wearable hybrids with laser diodes are your best options. Power output matters – look for at least 100–200 mW for home devices.
For skin health, acne, or hair growth – quality LED panels or masks are appropriate and cost-effective. Laser penetration advantage doesn’t apply at these surface targets. Focus on confirmed wavelengths (630–660 nm for skin, 650–670 nm for hair) and adequate irradiance data from the manufacturer.
For broad muscle recovery or full-body anti-inflammatory use – large LED panels or flexible pads covering significant surface area. Look for both red (660 nm) and near-infrared (850 nm) diodes.
For chronic joint conditions needing daily hands-free treatment – wearable devices. Check whether they use true laser diodes or LEDs, and whether the wavelengths match your target depth.
For cognitive support or brain health – transcranial PBM devices specifically. Don’t use a regular skin or pain device near the head and call it brain therapy – the devices are purpose-built for skull penetration.
Things to always check regardless of format:
- Wavelength listed in nm (not vague terms like “red light” without specifics)
- Irradiance data at actual treatment distance, not contact distance
- FDA clearance or registration (cleared is better than registered – it implies clinical evidence review)
- Return policy, because outcomes vary and you need time to evaluate
A Note on Safety and Contraindications
LLLT and PBM devices have a strong safety profile across the research literature. The therapy is non-invasive, non-thermal, and free of ionizing radiation. But a few cautions apply:
- Eye protection is essential with any device – laser or LED – particularly handheld units. Direct eye exposure from laser devices carries a genuine injury risk
- Don’t treat over active cancer or suspicious lesions without medical supervision
- Avoid use during pregnancy over the abdomen
- Check medications – some photosensitizing drugs (certain antibiotics, diuretics, psychiatric medications) can increase light sensitivity
- Higher-powered clinical laser units (Class 3B and Class 4) require professional supervision and safety protocols – these are not home devices
For most consumer-grade devices used as directed, adverse effects are rare and mild – occasional temporary redness or tingling at the treatment site.
Frequently Asked Questions
What is the difference between cold laser therapy and red light therapy?
A:Cold laser therapy (LLLT) uses focused, coherent laser diodes that penetrate deeper into tissue – up to 2–5 cm. Red light therapy typically refers to LED-based devices that affect more superficial tissue. Both work through photobiomodulation, but laser devices have a depth advantage for musculoskeletal and joint applications. For skin-level treatments, quality LED devices produce comparable outcomes.
Are LLLT devices FDA approved?
A: Some are. FDA-cleared LLLT devices have gone through a regulatory review demonstrating safety and efficacy for specific indications – this is the stronger standard. FDA-registered devices have simply been listed with the FDA. When a device claims clearance for a specific condition (pain relief, hair loss, wound healing), that carries more weight than simple registration.
What wavelength should I look for in a cold laser device?
A: For musculoskeletal pain and deep tissue: 808–850 nm near-infrared. For surface-level skin treatment: 630–660 nm red light. Many effective devices combine both. For transcranial brain applications: 810 nm or 1064 nm.
How long does it take for LLLT devices to work?
A: Most clinical trials show measurable improvements at 4–6 weeks with consistent use (3–5 sessions per week). Don’t judge a device for two weeks. Acute injuries may respond faster; chronic conditions typically take longer.
Can I use a cold laser device at home?
A: Yes – consumer-grade cold laser and LLLT devices are designed for home use. Lower-powered devices (Class 2 and Class 3R lasers, and LED devices) are safe for self-administration when used according to manufacturer instructions. High-powered clinical lasers (Class 3B and Class 4) should be used under professional supervision.
What are photobiomodulation devices used for?
A: The evidence-supported applications include: musculoskeletal pain and injury recovery, wound healing, hair loss (androgenetic alopecia), skin rejuvenation, acne, oral mucositis, dental pain, and emerging brain health applications via transcranial PBM. The breadth of conditions reflects the fundamental nature of the mechanism – mitochondrial stimulation affects cellular function across virtually all tissue types.
The Bottom Line
Cold laser therapy, LLLT, and photobiomodulation are the same category of treatment – just different names that accumulated over decades. The devices, however, are genuinely different. True laser devices and LED devices produce light through different mechanisms, with real consequences for penetration depth and best-fit applications.
The market is noisy and inconsistent with specifications, which makes it easy to spend money on the wrong thing. Know your target – surface or deep, local or broad, body or brain – and match the device format to it. Verify wavelengths, irradiance data, and FDA clearance rather than trusting marketing claims alone.
The underlying science is solid. The research base is large and growing. These devices, when matched correctly to the application and used consistently, represent one of the more well-supported non-pharmaceutical tools in the current wellness landscape.